This web page was produced as an assignment for Genetics 677, an undergraduate course at UW-Madison.
What is psoriasis?
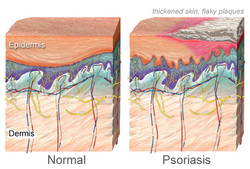
Psoriasis is a noncontagious, autoimmune disease causing inflammation of the skin. This disease affects the immune system causing outer skin cells (epidermis) to grow at an abnormally fast rate. Normally, skin cells are replaced every 4 weeks, but psoriatic skin replaces cells every 3-4 days (1). This causes a patchy rash of itchy, scaling skin (called plaques). Plaques are most commonly reported in the elbows, knees, and trunk region.
Psoriasis affects 2-3% of people with European descent (2). Several types of psoriasis exist, each affecting the skin differently in varied regions of the body, such as the scalp or body creases. The most common form is plaque psoriasis affecting 2-3% of Americans, most of them being adults (1). Other types include: guttate psoriasis, pustular psoriasis, inverse psoriasis, and erthrodermic psoriasis. The disease is also associated with psoriatic arthritis, a painful inflammation of the joints that can lead to joint destruction, which develops in about 15% of people having psoriasis (3). Individuals with the disease often suffer from societal discomfort and psychological disorders due to the difficulty of symptom management (5). Click here to learn what it is like to live with psoriasis.
Psoriasis affects 2-3% of people with European descent (2). Several types of psoriasis exist, each affecting the skin differently in varied regions of the body, such as the scalp or body creases. The most common form is plaque psoriasis affecting 2-3% of Americans, most of them being adults (1). Other types include: guttate psoriasis, pustular psoriasis, inverse psoriasis, and erthrodermic psoriasis. The disease is also associated with psoriatic arthritis, a painful inflammation of the joints that can lead to joint destruction, which develops in about 15% of people having psoriasis (3). Individuals with the disease often suffer from societal discomfort and psychological disorders due to the difficulty of symptom management (5). Click here to learn what it is like to live with psoriasis.
Treatments
To date, there is no cure for psoriasis, but treatments exist to relieve/control symptoms (1). Treatment approaches vary on the severity of the disease. Methods of treatments include: topical agents (often including steroids), phototherapies, oral systemic agents (pills), and immunomodulation therapies (6). Psoriasis treatments must be diligently used and often a combination and/or rotation of treatments are needed to manage symptoms. Click here to watch a video on how symptoms are managed with treatments.
Like many autoimmune diseases, symptom outbreaks arise from triggers. Triggers of psoriasis include: emotional stress, medications (lithium, beta-blockers, anti-malarials, etc.), skin injury or infections, and tobacco/alcohol usage (4). Avoiding triggers is a major component of symptom control.
Like many autoimmune diseases, symptom outbreaks arise from triggers. Triggers of psoriasis include: emotional stress, medications (lithium, beta-blockers, anti-malarials, etc.), skin injury or infections, and tobacco/alcohol usage (4). Avoiding triggers is a major component of symptom control.
What causes psoriasis?
Genetically speaking, it is still uncertain whether the defect lies in the immune system or the skin; however, there are risk factors identified in both, the immune system and the skin, that predispose someone to the disease. There are familial components of the disease; for example, if a sibling has psoriasis, ones’ chances of getting the disease are 4-6X higher (2). Overall, the heredity is very complex and still poorly understood. A better understanding of the disease will thus lead to better treatments and possibly a cure.
Psoriasis at the genetic level
Studies have identified an interval of DNA that contains a psoriasis susceptibility locus in a 300 kb region containing the major histocompatability complex (MHC) and more specifically the HLA-C (human leukocyte antigen C) region (8). This HLA-C region has unique high risk protein alleles, strongly associating this gene with psoriasis (8). Furthermore, this locus is the only locus that has continuously been associated with psoriasis (9).
HLAs function are to present peptides from digested proteins, from the inside of a cell. This is significant for proper immune function.
HLAs function are to present peptides from digested proteins, from the inside of a cell. This is significant for proper immune function.
References
1. Levine N M.D. (2010) "Understanding Psoriasis--the basics." WebMD.
2. Bhalerao J, Bowcock A. The genetics of psoriasis: a complex disorder of the skin and immune system. Hum Mol Genet. 1998;7:1537–1545.
3. Nograles KE, et al. New insights into the pathogenesis and genetics of psoriatic arthritis. Nat Clin Pract Rheum. 2009;5:83–91.
4. Rongioletti F, et al. Psoriasis induced or aggravated by drugs. The Journal of Rheumatology. 2009;83:59–61.
5. Esposito M, et al. An Italian study on psoriasis and depression. Dermatology. 2006. 212:126.
6. Armstrong A M.D. A review of health outcomes in patients with psoriasis. Dermatologic Clinics. 2012;30:1
7. Tiilikainen A, et al. Psoriasis and HLA-Cw6. Br J Dermatol. 1980;102:179–184.
8. Rajan N, et al. Sequence and haplotype analysis supports HLA-C as the psoriasis susceptibility 1 gene. Am J Hum Genet. 2006;78(5):827-51.
9. Bowcock, A and Krueger, J. Getting under the skin: the immunogenetics of psoriasis. Nature Reviews Immunology. 2005;5:699-711
2. Bhalerao J, Bowcock A. The genetics of psoriasis: a complex disorder of the skin and immune system. Hum Mol Genet. 1998;7:1537–1545.
3. Nograles KE, et al. New insights into the pathogenesis and genetics of psoriatic arthritis. Nat Clin Pract Rheum. 2009;5:83–91.
4. Rongioletti F, et al. Psoriasis induced or aggravated by drugs. The Journal of Rheumatology. 2009;83:59–61.
5. Esposito M, et al. An Italian study on psoriasis and depression. Dermatology. 2006. 212:126.
6. Armstrong A M.D. A review of health outcomes in patients with psoriasis. Dermatologic Clinics. 2012;30:1
7. Tiilikainen A, et al. Psoriasis and HLA-Cw6. Br J Dermatol. 1980;102:179–184.
8. Rajan N, et al. Sequence and haplotype analysis supports HLA-C as the psoriasis susceptibility 1 gene. Am J Hum Genet. 2006;78(5):827-51.
9. Bowcock, A and Krueger, J. Getting under the skin: the immunogenetics of psoriasis. Nature Reviews Immunology. 2005;5:699-711
Site created by Valeri Lapacek
Genetics 677 Assignment, Spring 2012
University of Wisconsin-Madison
Last Updated: 5/23/2012
Genetics 677 Assignment, Spring 2012
University of Wisconsin-Madison
Last Updated: 5/23/2012
